EOSINOPHILIC GASTRITIS, EOSINOPHILIC ENTERITIS, AND EOSINOPHILIC COLITIS
When increased numbers of eosinophils is observed in the stomach, the small intestine, or the large intestine, the patients are diagnosed with eosinophilic gastritis (EG), eosinophilic enteritis (EE), or eosinophilic colitis (EC), respectively.
These are rare disorders that affect less than one individual in 10,000 inhabitants. Symptoms depend on the affected organ:
- Eosinophilic gastritis: pain, nausea, vomiting, weight loss
- Eosinophilic enteritis: pain, diarrhea, malabsorption, weight loss, ascites
- Eosinophilic colitis: pain, diarrhea, ascites
Most patients are diagnosed between ages of 30 and 50 years. In contrast to EoE, the eosinophilic disorders of the stomach, small intestine, and colon are still poorly defined. Cutoff values for the microscopic diagnosis are about to be defined by an international consortium (CEGIR), in which several SNEGID members participate.
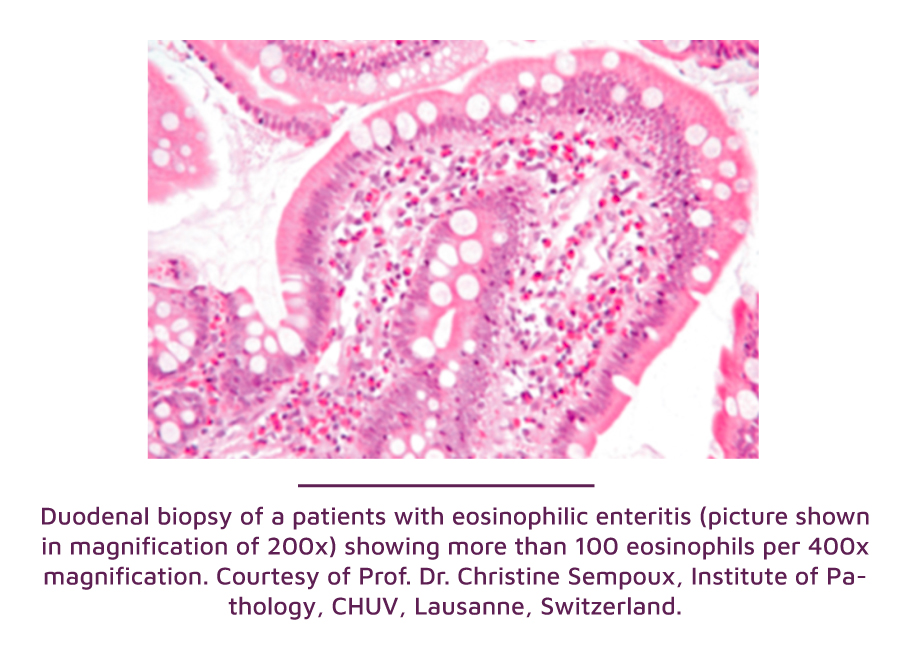
Food allergens seem to play a role in some of the affected patients. Diagnosis requires an endoscopy with biopsies to assess the eosinophil number in affected tissues. The endoscopic appearance is variable and ranges from a normal aspect to a reddening of the mucosa and ulcerations. Besides the endoscopic and laboratory workup, patients need imaging (mostly scanner) and a consultation with an allergist/immunologist and hematologist. Sometimes a consultation with a pneumologist and cardiologist is also necessary. The management of EGID manifestations requires a multidisciplinary team. Therapeutic approaches include steroids, immunomodulators, food elimination diets, and targeted biologic therapies against mediators active in eosinophil recruitment. The natural history of EG, EE, and EC still needs to be characterized.
The Swiss EoE Cohort is supported by the following entities: